Kenta Maeda was sent to the 10-day DL with a diagnosed right hip strain against the Phillies. In 2017, Maeda experienced left hamstring tightness, but got over that quickly. He acknowledged the right hip has been a lingering issue recently, but doesn't think it will keep him out too long.
Tale of the Tape:
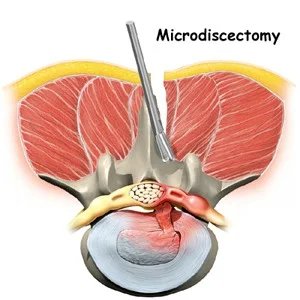
Watching him pitch and his stride when he walks, his pelvis already starts in a rotated position which makes it hard for him to follow through during the arm cocking and acceleration phases. He attempts to drive through the right hip, but hits a road block, forcing him to extend excessively through his trunk. As he tries to get more velocity, he attempts to force his right hip drive and rotate his pelvis out of his bad position. Muscles that have been in a shortened position for a while, lengthen under excessive load causing his hip muscles to strain. Over time, this can go from a muscle strain to joint pathology as it causes the ball in the socket to overcompensate and ride excessively forward for the lack of what the pelvis won't do.
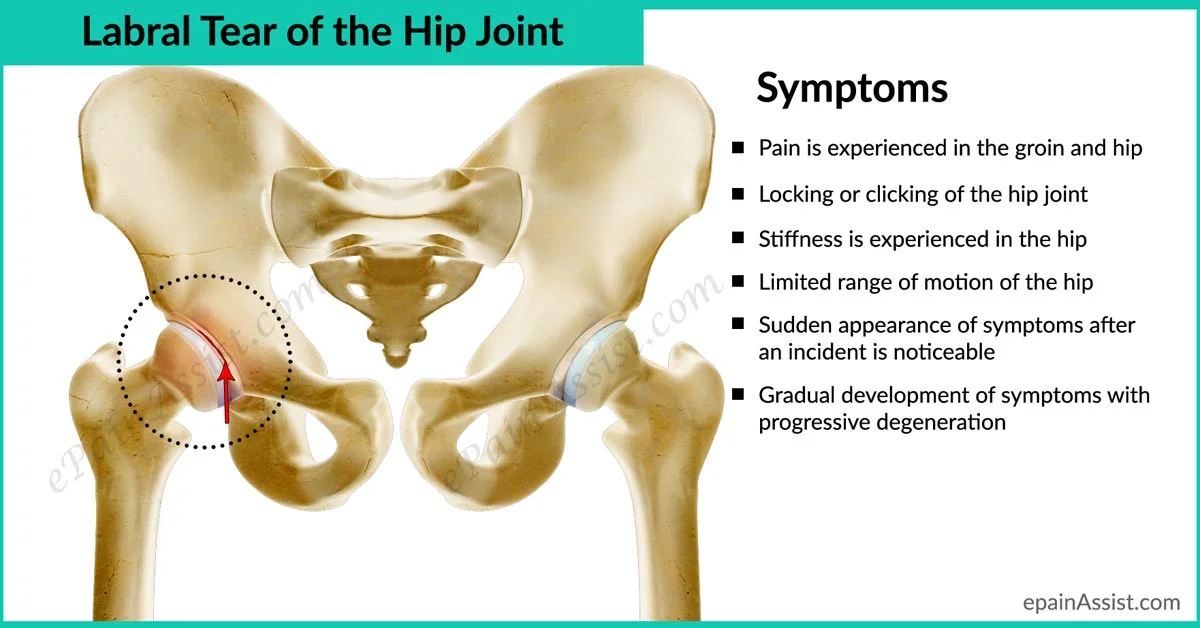
Synopsis: Maeda seems to be unphased by this recent hip injury and should be back on the mound after missing a start. This is a small impairment of the right lumobopelvic complex and can be fixed with a little work. But if this continues, it can cause right hip labral issues, back problems and right shoulder problems down the line. At the end of the day, if he wants to have healthy finishing pitching mechanics, he will need to address his starting position.
The Injury Analyst is a blog dedicated to not only explaining injuries that have occurred, but predicting and highlighting future injury risks for professional athletes. You can email us at info@jamsportsandspine.com
Note: I have not seen the subject of this article personally in clinic, rather all views and opinions of the author have been made based off of video footage of the athlete. This article is not meant as a diagnosis or a treatment plan.